
You Can’t Undo 9 Months in 30 Days: Pilates, DRA, and Reality.

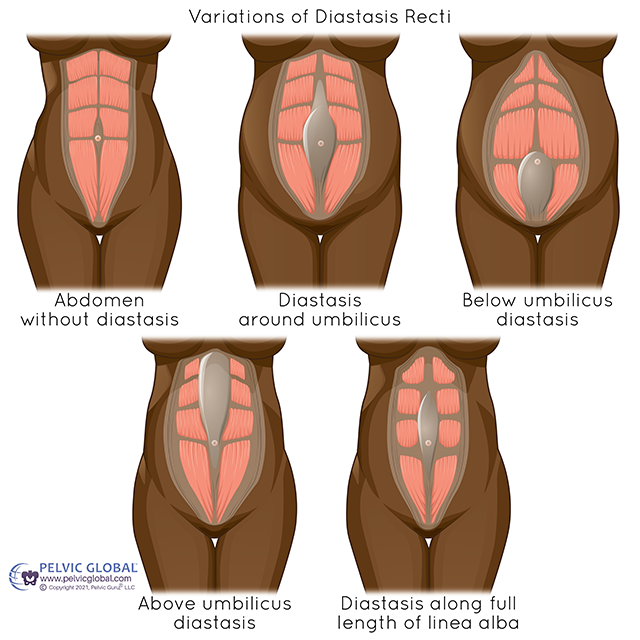
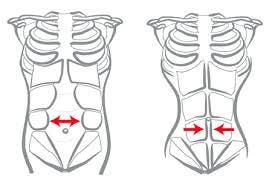
If you’ve ever Googled diastasis recti at 2 a.m., you already know the internet will have you believing your abdomen is either “ruined” or one $39 program away from being “snatched” by next Tuesday. Neither of those extremes is scientific, and neither is useful. Diastasis recti abdominis (DRA) is commonly described as the separation of the rectus abdominis muscles along the linea alba, often developing during pregnancy and the postpartum period due to mechanical stretch and hormonally mediated changes affecting connective tissue (Gruszczyńska & Truszczyńska-Baszak, 2018). Pilates is frequently recommended as a conservative approach, but “recommended” is not the same as “proven.” This synthesis asks a more precise question:
Does Pilates meaningfully reduce inter-recti distance (IRD) and improve abdominal function in populations experiencing DRA?
The most direct postpartum evidence supports the idea that a structured mat Pilates program can reduce IRD and improve abdominal performance, at least in the short term. In primiparous postpartum women, a 4-week mat Pilates program conducted at high frequency (50 minutes per session, 5 days per week) was associated with significant reductions in IRD and waist circumference and improved abdominal muscle endurance compared with controls (Lee et al., 2023). That matters because it suggests Pilates is not just “good for posture” in an abstract way; it can produce measurable changes when delivered with consistent dosage and clear progression (Lee et al., 2023).

There is also evidence that mat Pilates-based exercise may reduce IRD outside the early postpartum window, which is important for the many women who did not have “perfect” postpartum care, wrapping, rest, or rehab support. In climacteric women with DRA, a 12-week Pilates-based program reduced IRD across multiple abdominal regions (Silva et al., 2024). This population is not postpartum, so generalization requires caution, but the finding is still clinically relevant because it suggests that Pilates may influence IRD even when the body is operating under different hormonal conditions and timelines (Silva et al., 2024).
Smaller clinical reports are consistent with these outcomes, though they are not decisive on their own. A case report documenting mat Pilates in a primiparous postpartum woman observed reductions in IRD and improvements in trunk muscle endurance, aligning with the concept that Pilates-based training can improve both structural measures and functional capacity (Gahlot et al., 2024). Case reports cannot tell us what will happen for most people, but they often illustrate the “how” behind the observed improvements (Gahlot et al., 2024).
If we zoom out, Pilates falls within a broader family of interventions that target deep core coordination and trunk stabilization. A meta-analysis examining core stability exercise in postpartum women reported reductions in DRA measures using both caliper and ultrasound distances, supporting the overall premise that targeted stability training can reduce IRD (Oktaviyani et al., 2022). This is relevant because many programs labeled “Pilates-inspired” share overlapping elements with core stabilization protocols, including controlled breathing, progressive loading, and emphasis on deep abdominal engagement (Oktaviyani et al., 2022).
A literature review of exercise approaches for pregnant and postpartum women with DRA concludes that non-surgical, exercise-based interventions can reduce DRA, while also noting that current evidence does not establish one method as universally superior (Gruszczyńska & Truszczyńska-Baszak, 2018). That point is crucial because it reframes Pilates as a valid option within conservative care, rather than a singular miracle modality that must work for everyone in the same way (Gruszczyńska & Truszczyńska-Baszak, 2018).
Some studies also suggest that multimodal strategies may support conservative outcomes. For example, research on abdominal binders paired with strengthening exercises indicates improvement in postpartum DRA-related outcomes (Patwardhan et al., 2021). Although this is not Pilates-specific, it supports a practical clinical reality: for some individuals, external support plus progressive strengthening may be beneficial, and Pilates can operate as one structured strengthening approach within a broader plan (Patwardhan et al., 2021).
“Fixing” DRA: Anatomical Measures Versus Function
This is where the internet gets dramatic. Many discussions treat DRA as if it were real only when the “gap” closes, as if the body were a zipper and you needed the right trick. The literature is more nuanced. Changes in IRD are important, but functional outcomes, such as endurance, trunk stability, and symptom improvement, are also clinically meaningful and may not perfectly mirror IRD changes (Gruszczyńska & Truszczyńska-Baszak, 2018; Lee et al., 2023). In the Pilates study by Lee et al. (2023), improvements were not limited to IRD; waist circumference and abdominal endurance also improved, supporting the idea that Pilates may influence both structure and performance (Lee et al., 2023). From a conservative care perspective, this distinction matters because many women are seeking improved support, comfort, and confidence in movement outcomes that can be meaningful even when anatomical change is modest.
Variability, Measurement Issues, and Why the Results Don’t Always Match
The magnitude and durability of IRD reduction with Pilates-based exercise likely depend on postpartum stage, baseline severity, connective tissue tolerance, intervention dosage, and measurement method. Silva et al. (2024) report IRD reductions in climacteric women, but postpartum DRA involves different tissue conditions and remodeling contexts, so findings should not be treated as interchangeable (Silva et al., 2024). Meta-analytic findings also show variability in effect sizes and statistical significance across studies of core stability interventions, which reinforces the need for better-designed randomized trials with standardized protocols and consistent measurement strategies (Oktaviyani et al., 2022). In other words, the evidence supports Pilates as promising and clinically relevant, but it also supports honesty about heterogeneity in outcomes.
Clinical Implications
Based on available research, Pilates can be a valid conservative strategy for DRA management, particularly when implemented as a structured, progressive program emphasizing deep core coordination and controlled load exposure. The best-supported framing is that Pilates may reduce IRD for some individuals and can improve abdominal endurance and trunk stability, especially when dosage is sufficient and progression is appropriate (Lee et al., 2023; Oktaviyani et al., 2022). Because outcomes vary, Pilates is best presented as part of individualized conservative care, not as a guaranteed standalone fix for every presentation of DRA (Gruszczyńska & Truszczyńska-Baszak, 2018). Clinically, this suggests monitoring both structural measures (e.g., ultrasound or calipers) and functional outcomes (e.g., trunk endurance, symptom changes) to track meaningful progress, rather than relying solely on gap size (Lee et al., 2023).

De Resistance
Pilates appears to be a clinically reasonable conservative intervention for DRA, with evidence indicating potential reductions in IRD and improvements in abdominal endurance and trunk stability in postpartum and hormonally influenced populations (Gahlot et al., 2024; Lee et al., 2023; Oktaviyani et al., 2022; Silva et al., 2024). However, the extent of anatomical “fixing” varies, and the literature supports Pilates most strongly when it is delivered as a structured component of a broader core stabilization strategy that prioritizes deep core engagement and progressive loading (Gruszczyńska & Truszczyńska-Baszak, 2018; Patwardhan et al., 2021). The most evidence-consistent promise is not a guaranteed full closure of IRD for every person, but a meaningful improvement in abdominal wall function that many women experience as increased stability, reduced doming, and improved movement confidence over time (Lee et al., 2023).
References
Gahlot, P., Singh, R., & Shah, J. (2024). Ab. No. 113 Effects of mat Pilates program on inter-recti distance, waist circumference, and trunk muscle endurance in a primiparous woman with post-partum diastasis recti: A case report. Journal of Society of Indian Physiotherapists, 8(1), 74–75. https://doi.org/10.4103/jsip.jsip_abstract_58
Gruszczyńska, D., & Truszczyńska-Baszak, A. (2018). Exercises for pregnant and postpartum women with diastasis recti abdominis – Literature review. Advances in Rehabilitation, 32(3), 27–35. https://doi.org/10.5114/areh.2018.80967
Lee, N., Bae, Y., Fong, S., & Lee, W. (2023). Effects of Pilates on inter-recti distance, thickness of rectus abdominis, waist circumference, and abdominal muscle endurance in primiparous women. BMC Women’s Health, 23(1). https://doi.org/10.1186/s12905-023-02775-5
Oktaviyani, F., Pamungkasari, E., & Murti, B. (2022). Effect of core stability exercise in preventing diastasis recti abdominis among normal birth delivery postpartum mothers: A meta-analysis. Indonesian Journal of Medicine, 7(2), 188–199. https://doi.org/10.26911/theijmed.v7i2.536
Patwardhan, S., Pawar, V., & Patil, S. (2021). Effect of conventional abdominal binder on diastasis recti abdominis in post-partum women. Journal of Evolution of Medical and Dental Sciences, 10(30), 2255–2259. https://doi.org/10.14260/jemds/2021/461
Silva, E., Bortolli, T., Vesentini, G., & Marini, G. (2024). Effectiveness of Pilates-based exercises on the diastasis recti abdominis in climacteric women: A randomized controlled trial. ABCS Health Sciences, 49, e024207. https://doi.org/10.7322/abcshs.2022071.2135